
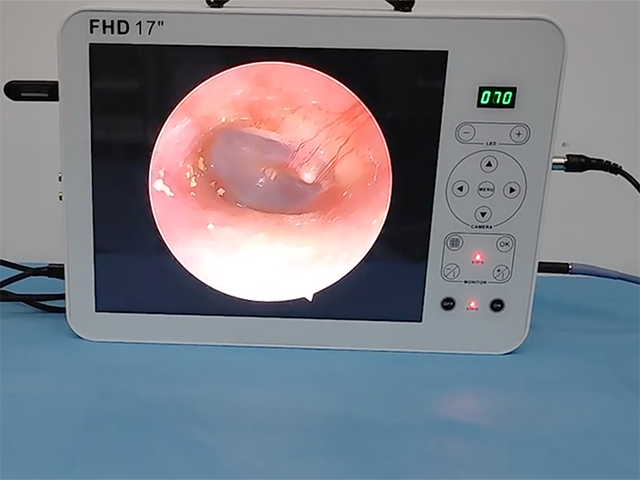
cystourethroscopy

01 Bleeding
Cystourethroscopy is an invasive examination, and gross hematuria often occurs after the operation, but the degree is usually not serious, no special treatment is required, and it usually resolves quickly. However, sometimes patients are severely injured due to urethral stricture, prostatic hyperplasia or rough operation, and the severity and duration of pain and hematuria also increase and prolong accordingly. Hematuria can also occur in people who have biopsies from bladder tumors or other diseases. However, most patients can still recover on their own under these conditions. Occasionally, severe hematuria or even blood clot fills the bladder. In this case, an indwelling three-lumen catheter may be required for bladder irrigation, and emergency surgery may even be required to remove the blood clot and/or treat the original disease.
02 Infection
Cystourethroscopy is an invasive procedure, and there is a certain risk of infection after surgery. It has been reported that 5% to 8% of patients develop bacteriuria after cystoscopy, and about 2% to 5% of patients can develop after cystoscopy. Urinary tract infection symptoms. There are three common reasons: ① urethral fever, even after cystourethroscopy, urethral fever may occur, and chills and high fever may appear in a short period of time. ②In the case of the original urinary tract infection, the infection may be aggravated after the operation. After retrograde angiography and other operations, it may also induce upper urinary tract infections such as acute pyelonephritis and empyema. ③ iatrogenic infection. The disinfection and aseptic operation of the instruments must be strictly performed. Prophylactic antibiotics can be used before the operation. After infection, sensitive antibiotics should be given in time, and attention should be paid to relieve the obstruction of the upper and lower urinary tracts to ensure the smooth drainage of urine.
03 Urethral injury
Urethral injury mostly occurs in patients with urethral obstruction, such as urethral stricture or benign prostatic hyperplasia. When it is difficult to enter the mirror and blindly and violently enter the mirror, it can cause urethral injury, and in severe cases, the urethra can be pierced to form a false tract, and even the bladder and rectum can be damaged. Therefore, before the examination, it is necessary to carefully understand the medical history and familiarize with the condition. The operation must be careful and gentle. When there is resistance, blind and violent insertion must not be performed. For patients with urethral stenosis or false tract formation, it may be necessary to use a thinner ureteroscope instead of cystoscope. It is safe to indwell a guide wire after entering the bladder smoothly under direct vision, and then dilate the urethra along the guide wire.
04 Bladder Injury
Bladder injury mostly occurs in patients with contracted bladder. For patients with bladder tuberculosis, bladder tumor after multiple treatments, and patients with anuria on dialysis, it is necessary to make a good prediction when performing cystourethroscopy to avoid inserting the endoscopic sheath too deeply. When bladder perforation has occurred, end the procedure as soon as possible to avoid continued flushing. According to the location of perforation, it can be divided into extraperitoneal and intraperitoneal types. For the intraperitoneal type, a small number of patients may still require surgical repair after indwelling catheters.
Ureteroscope

01 Perforation or avulsion of the ureter
With the advancement of ureteroscopy equipment and operating techniques, the probability of serious complications such as ureteral perforation during ureteroscopy has dropped to 0-4.7%, but ureteroscopy is still the most common cause of ureteral injury. The incidence is related to operating time and operator experience. It is important to note that the rigid ureteroscope can only be advanced if the lumen and safety wire are visible. When the ureter is stenotic and difficult to enter the mirror, do not force the mirror to avoid ureteral avulsion caused by the ureteral mucosa wrapping the mirror body.
02 Ureteral stricture
There is a risk of ureteral stricture after ureteroscopy, and avoiding intraoperative complications such as ureteral perforation and mucosal avulsion can reduce the probability of long-term postoperative ureteral stricture. Active use of ureteral stent drainage after ureteral mucosal injury can reduce the probability of ureteral stricture.
03 Infection
Special attention should be paid to ureteroscopy in patients with upper urinary tract obstruction or uncontrolled urinary tract infection. Interventional procedures and pressure during ureteroscopy may lead to bacteremia and sepsis. Preoperative precautions should be used. Antibiotics can reduce this risk. Attention should be paid to the perfusion pressure during the operation and effective renal drainage after the operation. Bacteremia and sepsis should be treated with intravenous antibiotics.








Leave A Inquiry